Labral tear
An injury to the labrum, the soft tissue that covers the ball and socket joint of the hip, is called a labral tear.
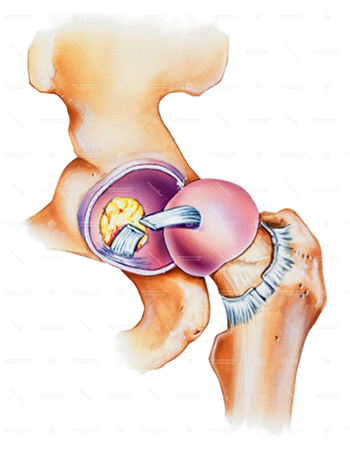
The hip is a ball and socket joint. The ball is the femoral head, located at the top of the thigh (femur) bone, and the socket is the acetabulum, which is part of the pelvis. Both are lined with cartilage allowing smooth movement without joint pain.
The ball and socket joint is sealed by soft tissue called the labrum creating a vacuum seal and suction effect, keeping the synovial joint fluid in place and protecting your joint cartilage during physical activity. An injury to the labrum is called a labral tear.
What is a labral tear?
Tears in the labrum often occur in patients in which there are pre-existing structural abnormalities (such as femoroacetabular (hip) impingement or hip dysplasia). Less often they occur after trauma, or over-usage during high-intensity repetitive activities such as pivoting sports (e.g. football, tennis or golf) or ballet dancing. Left unchecked, labral tears can progress and often the hip joint cartilage starts to peel off, leading to further damage within the joint and eventually arthritis.
Symptoms of a labral tear
If you had a labral tear you may experience sharp, knife-like, groin pain. This tends to occur in activities such as squats/lunges or getting in and out of a low car. The pain is usually activity-related initially but can be severe and disabling, affecting work, parenting, and leisure pursuits. As tears and symptoms progress, walking distance, standing or sitting for prolonged periods becomes more problematic.
Pain while sitting is another characteristic feature of labral tears. This could manifest itself with the inability to drive long distances or air travel. Other symptoms include a catching sensation or clicking, as well as your hip ‘giving way’. In some cases, pain may be located in other areas such as the buttock, in front of the thigh or on the side of the hip.
Diagnosis and treatment for labral tears
The diagnosis of labral tears is based on a thorough clinical history and examination as well X-rays, MRI and CT scans. By far, most labral tears are associated with Femoral acetabular (FAI) impingement and developmental dysplasia of the hip (DDH). Therefore, treatment involves addressing the underlying cause as well as the labral tear. In a General Practice study, 50% of young adults (aged 18-55) presenting with groin pain were suspected to have FAI.
Initial management involves rest, activity modification, and anti-inflammatory medication. After symptoms have settled, physiotherapy is especially important to stretch and strengthen muscles around the hip. Injections into the hip joint are frequently performed. This allows the surgeon to assess how much of the pain is coming from the hip joint and give the patient a pain-free interval to enable more effective physiotherapy.
If symptoms persist despite the above measures, then surgery may be indicated. This is usually in the form of keyhole surgery (arthroscopy). The torn labrum can be removed (debrided) or repaired. Recent scientific work has shown to have better results following repair of labrum rather than resection. Addressing the underlying cause involves removing the extra bone causing impingement or stabilising the labrum in hip dysplasia.
The most important advice one can give to patients considering treatment for their hip condition is to seek out a well trained young adult hip specialist who can explore in detail patients’ expectations and together devise a personalised plan to achieve the best possible outcome.